

Data Shows Sharps Safety In The Operating Room Remains A Persistent Problem
August 10, 2018By: Adeline Yi, Anzen™ Product Manager
A Review of Sharps Injuries in the Operating Room From 2002-2016
According to the Centers for Disease Control and Prevention (CDC), sharps injuries in non-surgical settings have decreased by 31.6 percent, while sharps injuries in surgical settings have increased by 6.5 percent from 2001 to 2006.1
While non-operating room injury rates have shown improvement, overall injury rates in the surgical setting have increased, where adoption of safety devices is limited compared to nonsurgical settings. This has vital implications because The Needlestick Safety and Prevention Act (NSPA) of 2001 was established to reduce the occurrence of all sharps injuries.
In an effort to raise sharps safety awareness, information networks such as EPINet and MSISS have published data from 2002-2016 to educate healthcare facilities and governing entities.
Exposure Prevention Information Network (EPINet)
The Exposure Prevention Information Network (EPINet) provides healthcare facilities with a standardized system for tracking occupational exposures that put healthcare staff at risk. At its core, EPINet data helps improve healthcare worker safety. By annually tracking data from employee incident reports on needle sticks and sharps injuries, EPINet analyzes their findings from three groups of healthcare facilities:
- Hospitals in the eastern half of the United States
- Hospitals in South Carolina that are members of Palmetto Hospital Trust Services (PHTS)
- Hospitals in the Pacific Northwest that are affiliated with the Providence Health System
Massachusetts Sharps Injury Surveillance System (MSISS)
The Massachusetts Sharps Injury Surveillance System (MSISS) was established under the Massachusetts Department of Public Health (MDPH) after enacting regulations for sharps injury surveillance and prevention. MDPH requires all licensed acute and non-acute care hospitals to use devices with sharps injury prevention features as a provision of patient care. All hospitals must also submit an Annual Summary of Sharps Injuries to MDPH.
From there, MSISS publishes findings about occupations, devices, procedures and departments that are at risk for sharps injuries. It also shares information about challenges and successful prevention strategies with hospitals and healthcare workers in Massachusetts. All healthcare workers in MDPH licensed hospitals are included in the data.
The Massachusetts Department of Public Health regards operating room safety a “persistent issue” and highlights “the importance of selecting the most effective device, improved training in the use of these devices and improved product design, specifically the mechanism of the sharps injury prevention feature (e.g., shielding, retracting, sheathing)”2
Let’s take a look at the number of sharps injuries reported by EPINet and MSISS from 2002-2016:
MSISS
- In 2002, there were 3,413 injuries, with 921.51 occurring in the operating room.
- In 2015, there were 2,866 injuries, with 945.78 occurring in the operating room.
The graph below shows the number of injuries reported by MSISS from 2002-2015. The data shows that the number of injuries in the non-surgical setting has decreased over the years, while the number of injuries in the surgical setting has remained relatively constant.

EPINet
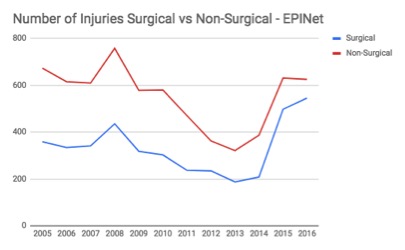
- In 2005, there were 1,033 injuries, with 359.48 occurring in the operating room.
- In 2016, there were 1,171 injuries, with 545.69 occurring in the operating room.
The graph below shows the number of injuries reported by EPINet from 2005-2016. The data shows that there was an overall downward trend in sharps injuries from 2005-2013, with non-surgical sharps injuries declining at a faster rate than surgical sharps injuries. However, from 2014 to 2016, there has been a sharp increase in the overall number of sharps injuries, with surgical sharps injuries increasing at a greater pace than non-surgical sharps injuries.
Data from both EPINet and MSISS suggest that sharps injuries in the surgical setting continues to remain a problem. Of vital concern is that most facilities do not offer safety scalpels or other safety surgical blades as an option, despite the statistics. This points to the need for an optimal safety scalpel to help reduce the risk in the operating room. By looking at objective data that spans a 14 year period, we can uncover the areas that need improvement and address the sharps safety concerns of today.
1 https://www.cdc.gov/niosh/stopsticks/sharpsinjuries.html
2 Overview of Sharps Injuries Among Hospital Workers in Massachusetts. Massachusetts Sharps Injury Surveillance System. August 2017. https://www.mass.gov/files/documents/2016/09/vb/sharps-injuries-hospital-workers-2002-2014.pdf